Patellofemoral Pain Syndrome

Patellofemoral Pain Syndrome is a very common type of knee pain felt around and under the kneecap. Here are tips to manage the pain of PFPS:
1. Rest
The first step is to avoid activities that stress the knee. That’s often anything involving a bent knee. This can include stairs, squatting, sitting with bent knees, walking, running, cycling, and even swimming.
Work out the activities that bring on your symptoms and rest as much as possible from them. Two weeks would be the minimum period of rest for mild cases. After this time, start testing your knees by slowly returning to normal activities. If symptoms return quickly, you will need to stop and rest for a longer period.
2. What about exercise?
Slowly reintroduce exercises so your knee can adapt to stress again. Start with exercises that keep the knee straight (see Quadriceps Setting). Exercises should not aggravate the pain. If you over-do it, try reducing the speed, resistance, amount of repetitions or the range of motion you move through.
Strengthening exercises for both the knee and hip have shown in studies to improve pain levels and function (1). Make sure to do exercises on both legs, not just the painful side.
Good exercises for the two weeks after the period of rest include:
· Quadriceps Setting: keep the leg straight, or only slightly bent and clench the muscles in your thigh for 3 seconds. Start slowly and gently, and increase the duration and strength of contraction as you improve. Aim for 3 sets of 10 clenches daily.
· Hamstring curls: an exercise to do at the gym. Lying face down, bend your knees up to 90˚ to strengthen the hamstrings
· Straight leg raise: lay on your back, turn your foot slightly outwards and lift your leg to approximately 45˚ off the ground without bending your knee. Hold for 2 seconds, then return it to the ground. Stop when your muscles fatigue, or you start to feel any pain.
· Sidelying straight leg raise: a harder version of a clam*. Lay on your side with your body in a straight line. Lift the top leg off the bottom one up to about 45˚ and hold for 2 seconds. Stop when your muscles fatigue, or you start to feel any pain.
Avoid exercises like deep squats or the leg press machine until you have noticed substantial recovery
3. Other Ideas
If you sit down during the day, try to sit with your knees only slightly bent to reduce the amount of pressure through the knee cap.
If you are a runner, try to avoid running on hard surfaces, and avoid slow paced running
Ice or heat can be used for pain relief to soothe sore knees
Massage or osteopathic treatment may help to relieve some flow-on effects of knee pain, like stiffness and soreness.
Knee strapping or braces can help to support the knee short-term
*I have put clams out of the main body as this exercise can create irritation in the buttocks and tighten the low back. If you can complete this without irritation:
Clams: lay on your side with both knees bent so your feet are in line with your spine. Lift the top knee off the bottom on, like opening a clam shell. Hold for 2 seconds, and repeat until your muscles fatigue or you feel any pain.
(1) Peters JS, Tyson NL. Proximal exercises are effective in treating patellofemoral pain syndrome: a systematic review. Int J Sports Phys Ther. 2013 Oct;8(5):689–700
What's my age again?

There is a constant that we ALL can't avoid. We will all get older. BAM - there it is! Sorry to say, no amount of ancient Tibetan anti-ageing, chakra cleansing, raw shea milk baths or organic gogi berry, wheat grass or metabolic blast juice shakes will change this fact. But if it feels good, and you feel good, then knock yourselves out. I might join you.
But let's face it some WILL age better than others for lots of different reasons. Some people are genetically blessed to age gracefully with little to no major health problems. Is this strictly due to the genes they were born with? Or are they doing something different to the rest of us, to EXPRESS better function of their genes?
Gene expression refers to a complex series of processes in which the information encoded in a gene is used to produce a functional product such as a protein that's required for optimal cell function (1). Gene expression is constantly being regulated by multiple metabolic, environmental and physiological factors.
I recently a saw BBC One TV show entitled "How to Stay Young". There was an interesting piece on how your general strength and mobility can be a predictor for long term health. Watch it here.
I had a go (and so should you so if you haven't watched it yet). I didn't do too badly, but my hip mobility is clearly a bigger issue than I first thought. If I'm going to age gracefully then I'll need to start working harder. Eating better, sleeping more, drinking less, seeing friends and of course moving better. We can't stop working hard at any of it and we might be able to prevent as many "age related" diseases as we possibly can.
Because I'm an Osteopath, the structure of every part of the human body and if they function well has always been my bag. But even more important is how all those body parts move and function when we walk, sit, swing, sing, poop, and breathe. Let alone when we want to lift a heavy weight over our head or sit for the majority of our life.
Our genes express themselves a lot better if we give them a good grease and oil change everyday. Katy Bowman from Nutritious Movement has pieced together some excellent information about why we need to move to keep our cells healthy and our genes expressing themselves optimally, which hopefully results in our bodies ageing the best they possibly can.
There is a lot of information around optimal human movement and over the next few BLOGs I will try to draw out some of the movements we need to work on getting better at, and because it's my BLOG let's start with my hips.
So What's Your Age Again? Do you plan on being young of mind, body and heart?
We are are all as old as we feel. Lucky we can all feel younger.
1. http://www.news-medical.net/life-sciences/Gene-Expression-An-Overview.aspx
Nerves and Radicular Pain (ridiculous pain)
Nerves are NOT invisible
Put simply, I used to think that nerves were microscopic. This was before I knuckled down to five years of study at University. Now I know that every part of the body has a nerve supply and you don’t need a microscope to see them. It all starts from our brain, moves onto our spinal cord and then nerves branch off and travel outward to EVERYTHING and when you put it all together it’s known as the nervous system.
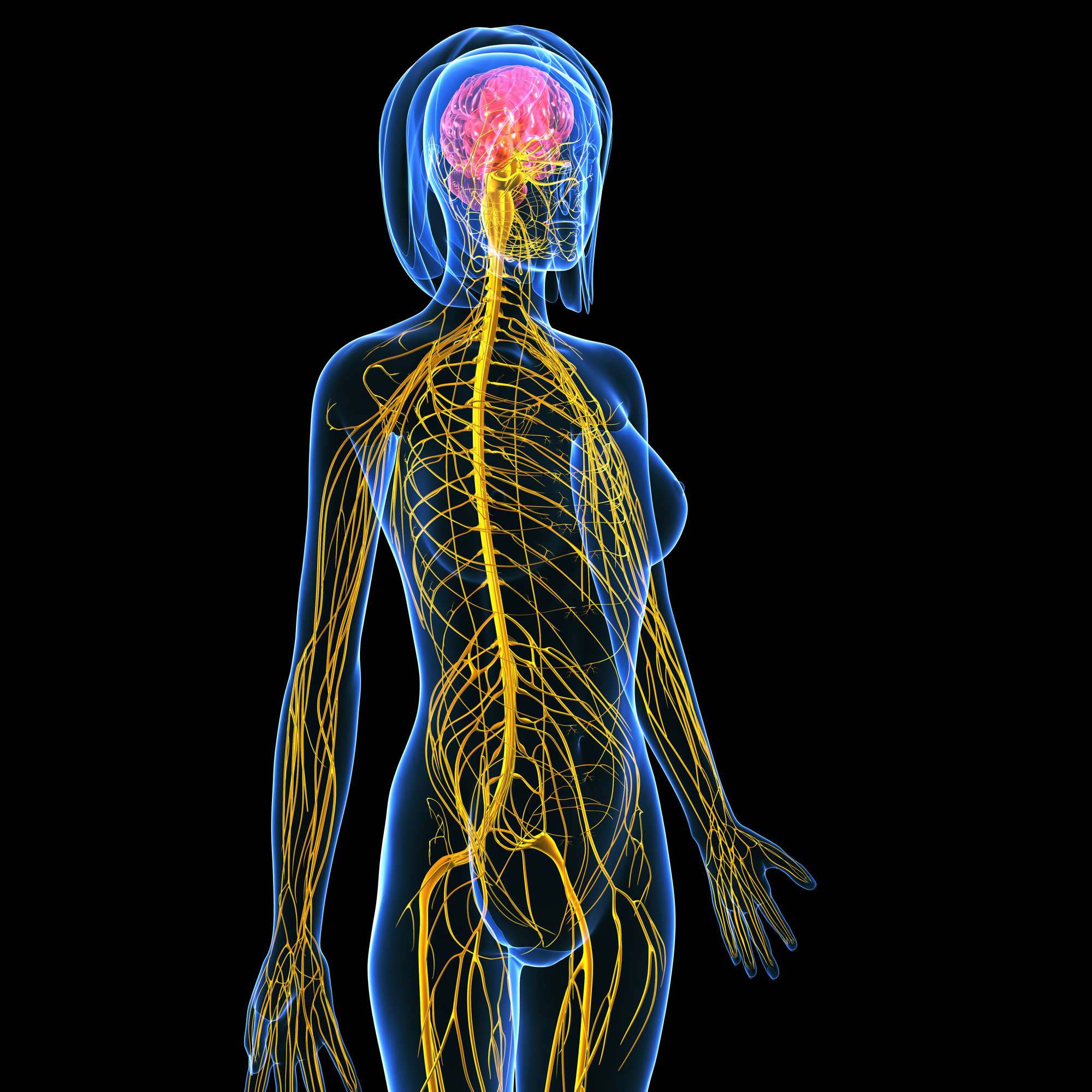
The nervous system is super important
Potentially, I can’t overestimate the importance of the nervous system. We would be a gelatinous blob without it. It manages 100% of everything, 100% of the time and it’s hungry for oxygen and glucose and if it doesn’t get these things it sends danger signals to our brain very quickly so that we can do something about getting them what they need. Normally this will involve fairly basic tasks like moving, moving so we can get something to eat and moving so that we can go somewhere to lay our head and go to sleep.
The nervous system is super sensitive
The 72 kilometres of nerves in our body exist to relay signals/information from bits of our body to the brain or from our pink, squishy brain out to bits of our body. These wonderful information carriers are sensitive to everything; chemicals, touch, movement, they are constantly monitoring every little thing about us. A short distance away from where the nerve exits the spinal cord, there is a very sensitive part that if entrapped or irritated by specific chemicals this may cause increased activity of that nerve. Increased activity means the nerve sends off lots and lots of information to the spinal cord and brain, which you might detect as pain or altered sensation in the skin.
This is what is known as ‘radicular pain’ as it ‘radiates’ through the body, most likely into our arm or leg, along the pathway of a nerve that has exited the spinal cord at your neck or lower down in the spine.
People will present to the clinic with pain into the arm or leg that seems to follow a pathway down a specific area. Radicular pain can present differently for different people. It may be felt as numbness and tingling, or burning pain, or a sharp, jabbing pain, or electric-shock like pain or extreme sensitivity to touch. When a nerve that exits the spinal cord in the low back, commonly radicular pain will be a gnawing, constant pain in their bum.
Who gets radicular pain?
It is estimated that between 13-40% of people will experience radicular pain at some point in their lives. There is a link to age, with the highest number of cases occurring between 40-50 years of age, and genetics may predispose this condition (1).
Is it my job's fault?
Some jobs seem to contribute to the development of radicular pain, such as working in awkward positions where the body is bent or twisted, with your hands above shoulders or when driving for prolonged periods. Equally, sitting a lot is starting to gain momentum as a risk factor for all sorts of conditions, including radicular pain. Smoking also increases the risk of radicular pain, as it alters the metabolic balance within the tissues of the spine (1).
If I have it, what can I do about it?
Most patients with radicular pain experience some improvement within four weeks from the onset of pain (2). The majority of cases resolve spontaneously with a multi-modal approach of pain relief such as anti-inflammatories or opioid based medication (1) and other more conservative measures, like manual and physical therapy or pain education (3). A number of studies supports the theory that a combination of treatments can lead to better outcomes (i.e. less pain) after three months, when compared to patients receiving either medication or physical therapy alone (4).
Can’t you just inject it? Or cut something out?
A 2014 review of research on radicular pain recommends that patients try 4-8 weeks of conservative treatment, before seeking more invasive interventions like spinal injections or surgery (5). It may seem like a long time to wait, especially when pain may cause difficulty sleeping, or reduce our ability to concentrate or enjoy even the most simple things in life.
Osteopathic Intervention
Manual therapy techniques along with exercise based rehabilitation is at least as effective as surgery for radicular pain (5) without the negative side effects. It’s frustrating but learning about what is happening, knowing the prognosis and enjoying even brief episodes of relief can provide hope and keep people focused on the light at the end of the tunnel.
Your osteopath can provide further information on these options. Book online to make a appointment.
(1) Woods, B.I & Hilibrand, A.S. (2015). Cervical radiculopathy: epidemiology, etiology, diagnosis and treatment. Journal of Spinal Disorders & Techniques, 28(5), 251-259
(2) V. J., Lubelski, D., Steinmetz, M. P., Benzel, E. C., & Mroz, T. E. (2014). Optimal Duration of Conservative Management Prior to Surgery for Cervical and Lumbar Radiculopathy: A Literature Review. Global Spine Journal,4(4), 279–286.
(3) Clark, C.L., C.G. Ryan, et al (2011). “Pain neurophysiology education for the management of individuals with chronic low back pain: systematic review and meta-analysis.” Manual Therapy 16 (6): 544-549.
(4) Cohen, S.P., Hayek, S., Semenov, M.A., Pasquina, P.F., White, R.L., Veizi, E., Huang, J.H.Y., Kurihara, C., Zhao, Z. et al. (2014). Epidural steroid injections, conservative treatment, or combination treatment for cervical radicular pain: a multicentre, randomized, comparative-effectiveness study. Anesthesiology, 121, 1045-1055.
(5) Boyles, R., Toy, P., Mellon, J., Hayes, M., & Hammer, B. (2011). Effectiveness of manual physical therapy in the treatment of cervical radiculopathy: a systematic review. The Journal of Manual & Manipulative Therapy, 19(3), 135–142.
This article was a combined effort of Angie Bruce and Cat Burns. Angie was the one who admitted she thought nerves were invisible and Cat provided the bulk of the sensible information and academic references.
Migraine Management

I recently attended a presentation on Migraine by Associate Professor and neurologist David Williams from Monash University. It was a worthwhile update hosted by Headache Australia at the Alfred Hospital. This blog does not replace information provided by your GP or specialist. The following is a summary of the information that was presented.
WHO SUFFERS FROM MIGRAINE?
About 15% of the population suffers from migraine at some stage in their lives.
WHAT IS MIGRAINE?
The most recent theory is that migraine is on the normal physiological spectrum i.e. all humans can suffer a seizure but not all have epilepsy.
The PROCESS of migraine is a complex and temporary chemical and electrical change in the brain that results in symptoms. It tends to start at the base of the brain (the brainstem) and moves like a tide involving the rest of the brain.
https://www.youtube.com/watch?v=pUbXB8vT8fY
http://makethislookawesome.blogspot.com.au/2011/11/what-is-migraine.html
HOW DO YOU KNOW IF IT'S MIGRAINE?
Simple test: If you have a headache and you shake your head and it gets worse then it's a migraine type headache.
TRIGGERS
They are different for everyone.
Commonly reported FOOD Triggers = chocolate, cheese, coffee, nuts, citrus, processed meats, MSG and aspartame, alcohol.
Commonly reported OTHER triggers: bright or flickering light, motion, loud sounds, strong odours, changes in atmospheric pressure, fatigue, lack of sleep, stress, hormones, skipping meals, some medication.
THE FOUR PHASES OF MIGRAINE
1. PRODROME/PREMONITORY: pre-symptomatic stage, e.g. not feeling right, brain fog, frequent and severe yawning, short tempered
2. AURA*: temporary spread of chemical changes to 50-60% of the brain
3. HEADACHE/PAIN
4. POSTDROMAL/RESOLUTION: the pain has passed, but you are left feeling fatigued and washed out
* Only 20-30% of people experience AURA symptoms e.g. visual scotoma (blind spots), blindness, speech disturbance, tingling, weakness, nausea, unsteadiness
PROGNOSIS
Migraines usually last a few days.
WHY? WHY? WHY?
Most people have a genetic vulnerability. In other words, it's how you're wired.
Nerves and blood vessels become sensitised to pain
Pain breeds pain
And the tissues are not as good at resetting after the pain has past
RESEARCH
Pain threshold is lower in people with migraines (pin pricks)
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3268359/
The same process occurs in low back pain:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3598908/
MEDICATION
There is NO evidence for pain medication which means NO panadeine NO paracetamol
WHY NO MEDICATION?
Rebound Headaches can occur with migraine
These can be caused by high rates of codeine overuse (Australia one of the only places it is available over the counter)
Triptans can be overused and this prevents the brain to allow the tide of pain to recede on its own
STOP the spread of chemical changes in the brain with NSAID and TRIPTANS
Preventers* = Endep, Topamax, Epilin
*Pharmaceutical preventers have multiple side effects as they change brain chemistry e.g. sedation, confusion, unsteadiness, nausea
* Nutritional preventers e.g. Vit B2, Mg, B2 Folate, Coenzyme Q10 - very individual.
YOU MUST HAVE A PLAN
1) Know YOUR migraine (at some point you must keep a migraine diary to plot evolution of symptoms)
2) Avoid triggers (PERSONAL)
3) Have an ACUTE MIGRAINE PLAN and HIT IT HARD (escalation of treatment) MUST catch it early, once headache is there (Phase 3) the chemical spread through the brain is TOO big
Step 1) HYDRATE (sleep/eat)
If this fails:
Step 2) NSAIDS e.g. voltaren, aspirin, ibuprofen
If this fails:
Step 3) Second dose NSAIDS (within shortened time period)
If this fails:
Step 4) TRIPTANS* maxalt, immigrin, naramig
If this fails after 2-3 days of headache/vomiting:
Step 5) HOSPITAL fluid infusions, stematol (anti-nausea) morphine
*Triptans can cause rebound headache
THERE IS NO ‘OFF THE SHELF’ TREATMENT
Be healthy - eat well, rest
Acceptance
Often natural fluctuations
Exercise
Good sleep hygiene (http://www.fairfieldosteo.com.au/reconstructinghealth/2015/7/2/five-tips-for-a-better-nights-sleep )
Intellectual stimulation
Good social network
Order of Important people
YOU
Family
Employer
GP
Nurse
Pharmacist
Specialist
Allied Health (combination of treatment that makes sense and is financially viable)
What is CHRONIC MIGRAINE?
CHRONIC MIGRAINE is an escalating episodic migraine and is vaguely classified as suffering with symptoms for more than 14 days per month.10% of sufferers fluctuate into chronic migraine at any given time2-3% of migraine sufferers find their pain becomes disabling.
Tell me about BOTOX?
Clinical trials suggest that BOTOX injections over seven key areas of the head and neck (31 total injection sites) can reduce the sensitisation process in people with CHRONIC MIGRAINE and return people to episodic migraine.
Top Tips for staying well this Christmas
Thanks to Vicki from Harvest Health for these tips.

Manage your diary
Although it can be difficult with work commitments, social engagements or children’s activities, try to schedule some downtime each week. Even a 20 minute walk around your local park can help you relax.
Breathe
Often when we’re rushing around we’re unconsciously taking short shallow breaths. Take a few moments to be mindful and focus on your breath. Make your breath slower and deeper through your nostrils. Breathe in for four counts and then out for four counts. Feel the difference within minutes during this simple mindfulness exercise.
Stay hydrated
It's at this time of year, when for many people, alcohol intake goes up. This can be exacerbated on a hot day. If you’re going out, remember the old rule of having a glass of water for every glass of alcohol. Add to this a big glass of water to start the day and another when you get home of an evening.
Prioritise sleep
To avoid becoming stressed and grumpy this time of year, regular good nights of sleep are essential. A good idea is to make a strict bedtime rule for yourself on those nights when you’re not going to be out.
Love your liver
The extra alcohol and processed or fatty foods that come with celebratory occasions means some extra work for your liver. Try the following to give your liver some support:
- Have at least 2-3 alcohol free days a week
- Take St Mary’s thistle, a herb which protects liver cells.
- Eat a small salad of bitter green leafy vegies.
Spend time outdoors
Make an effort to spend some time outside in a park, the countryside or even weeding your own backyard. It’s amazing how much more calm and centred we feel after spending time outdoors.
Eat your vegies
Balance the festive food by making yourself a couple of dinners each week that are simple, but full of vegetables and salad. And remember to reach for the veggie sticks at festive occasions.
Drink herbal tea
Take the time to enjoy the ritual of making yourself a cup of tea. Include relaxing herbs such as chamomile, lemon balm, lime blossom, oat straw, skullcap and lavender.
Take Stock
These tips make sense for every period of our life. If you've got a New Year's Resolution list nearby, and health isn't on your list, it's time to re-evaluate and consider making your health one of your top priorities for 2016.
Blocked Drains?

Manual Lymphatic Drainage
Manual Lymphatic Drainage (MLD) is an interesting example of a specific massage technique. It is purported to reduce swelling and is used to treat patients suffering from lymphoedema, or swelling of one or more limbs.
Lymphoedema can occur due to compromise or partial failure of the lymphatic system.
WHAT IS THE LYMPHATIC SYSTEM?
The lymphatic system is a complex network of tiny channels throughout the entire body. It’s primary function is drainage, circulation and filtration of fluid throughout the body and it also plays a significant role in immune response. In general, movement of the body creates the “pumping action” required to propel lymphatic fluid through this system.
Occasionally, underlying factors reduce the ability of the body to remove fluid. Factors including medication, disease, pregnancy, excessive weight or trauma. It is also frequently seen as a complication of mastectomy after lymph node removal or other surgical procedures.
WHAT HAPPENS IN AN MLD TREATMENT
MLD is a specialised technique in some practitioners’ tool belts. It is a fairly technical process and practiced by no more than a few hundred therapists in Australia. Petra Miliankos, the Myotherapist at Fairfield Osteopathic Clinic, outlines her approach to MLD:
“When the body gets into the position of not being able to clear fluid on it’s own, an external force (in this case a qualified human) can help remove the barriers to fluid removal.
When you learn MLD you study the movement of fluid along the channels from the tips of the toes and fingers in toward the main ducts in the pelvis and torso. By applying precise, gentle, rhythmic strokes along lymphatic pathways you can help move fluid through the channels.”
WHAT DOES THE RESEARCH SAY?
STUDY OF FOUR WEEKS OF MLD TREATMENT
One study (1) followed short-term MLD (over four weeks) and showed it can ameliorate chronic venous insufficiency severity, oedema, symptoms (fatigue and heaviness), pain and quality of life. Interestingly, the changes you might normally measure like range of motion, leg volume and strength showed no improvement. Quality of life measurements are extremely important, especially for the patient, and are often overlooked in studies.
But wait - doesn’t everyone feels better for a short time after a hands on treatment? True, however the patients in this study reported continued improvement four weeks after the last treatment. Petra said this confirms her experience:
“Anecdotally, clients report feeling better despite not meeting a drastic reduction in limb size. But this perceptual shift can be an important step towards self-management. A recent example is after only three treatments one of my clients felt significantly more mobile and confident enough to pursue an increase in exercise. She is now swimming twice a week at Northcote Pool. I’d say that’s a very positive outcome.”
FURTHER RESEARCH?
A 2015 literature review (2) confirmed the mixed outcomes in the evidence for MLD. There remains no gold standard protocols for the treatment of lymphoedema, so an individualised and clinically reasoned approach, like MLD, remains a valid option.
If you would like to speak to Petra to discuss whether MLD might benefit you, please call the clinic on 03 9489 0981 or book online.
(1) Dos Santos Crisotomo, R.S., Costa, D.S.A., de Luz Belo Martins, C., Fernandes, T.I.R., Armada-da-Silva, P.A. (2015). Influence of Manual Lymphatic Drainage on Health-Related Quality of Life and Symptoms of Chronic Venous Insufficiency: A Randomized Controlled Trial. Archives of Physical Medicine and Rehabilitation, 96(2); 283-291
(2) Finnane, A., Janda, M., & Hayes, S.C. (2015). Review of the evidence of lymphedema treatment effect. American Journal of Physical Medicine & Rehabilitation, 94(6): 483-498
Blurred Lines of Health Care

I felt the need to share the case of a patient I had recently. The issue is not with the patient themselves but with the care they received from another practitioner.
The mature gentleman in question had presented to me with a long history of knee pain. Due to that long history he had also developed some compensatory pain in the hip and low back as his overall function had diminished. Some treatment helped with the presenting complaint but the knee was still pretty bad. A quick consultation with the GP and it was agreed a specialist referral would be necessary. Turns out the knee was severely degenerated and he was a strong candidate for knee replacement surgery.
The patient was not keen on surgery, which is fair enough. The recommendation is always to hold out for replacement surgery as long as possible and I support that wherever possible. He decided to get a second opinion from another manual therapist, a Chiropractor, that had been strongly recommended by a friend of his. This opinion was meant to see if any more could be done to prevent surgery. I would always encourage a client to seek further advice if they have any doubts at all.
A COUPLE OF WEEKS LATER....
The patient returned to my practice a couple of weeks later with a full spinal X-ray series - from head to bum basically. They wanted my opinion on this series of X-rays that the Chiropractor had ordered. The patient was particularly interested in my opinion of their neck X-ray. There was a little bit going on in the neck but nothing too sinister at all. I asked whether they currently had neck pain. The answer was a resounding "No". Turns out they hadn't had any neck pain at the time of the X-rays either. However the Chiropractor had pointed out a lot of areas of 'concern' that would need to be addressed in a series of treatments over the next YEAR!
I'm sorry, but there was no pain and no clinical indication to X-ray anything above the knee in the first place. The Chiropractor may have valid reasoning in their own mind for pursuing a course of treatment on an asymptomatic neck but it's not good health care.
THE BUSINESS OF HEALTH CARE
A big problem with private practice health care is that it is about the practitioner's livelihood. There are mortgages, living costs and often large educational debts to pay for, as well as their own health care needs, and the list goes on. Many get into health care professions with the most noble of intentions only to find it is not that easy to make a living - not as easy or lucrative as many would think. There are numerous health care business coaches out there who wax lyrical about the money that can be made in private practice. Unfortunately, it is completely driven by increasing treatment for patients and this means they aren't always selling good health care in order to build those numbers. They are selling over treatment and dis-empowerment of the patient and that's not an equation we like too much.
A multitude of practitioners sign people onto treatments they don't need. In fact Four Corners did an hour long expose of the billions wasted in unnecessary investigations and treatments within the medical system.
http://www.abc.net.au/4corners/stories/2015/09/28/4318883.htm
Instead of the public purse paying for treatments it is the patient's personal income that pays for unnecessary treatments and for what end?
Practitioners may unknowingly prescribe snake oil. They have invested a lot in their careers and they may be dissatisfied with their earning potential or they may have chosen to ignore the evidence to everyone's peril.
HCF PROFILE
HCF is a private health fund that sends us the data comparing the number of treatments we provide to their members compared to other Osteopaths in the area. Providers at Fairfield Osteopathic Clinic provide 30% less treatment per person. I don't think it's limited to clients who are members of HCF!
And don't get me wrong, I don't think it's because we're more talented. I think it's because we take time to explain the complexities of pain, encourage clients to be insightful about their condition, and encourage an active care approach and more than anything empower our patients with the confidence and knowledge to help themselves on a daily basis.
Another thing we do is to ask what your goal is? Most of the time it's simple things; to get a better sleep, to be able to run with no pain, etc. Not many people are aiming for one hundred percent. There is no finish line or silver bullet. Reducing pain and improving function is maddeningly provisional and a lot of the time we are just there to give you a better chance of doing it better the next day.
This is not something that works for every patient. Some people benefit hugely from therapeutic touch for lots of different reasons and they seek hands-on treatment much more often than others. As long as patient and practitioner have a clear understanding of the care plan going forward then that is entirely appropriate.
OUTCOMES NOT OUTPUTS
All practitioners at Fairfield Osteopathic Clinic look at the outcomes for our patients, not at the outputs on the books. It's a terrible business model of course. So please, unless it's an exercise program, don't sign on for anything that's going to take twelve months.
* For interest of privacy many details have been changed.
To Gel or not to Gel? That is the question.

I have thought for years that topical gels were no better than placebo but after looking at the research I've had to challenge at least some of my opinions. Perhaps this will change (or at least inform) your mind.
Should I use Voltaren (Flector) Gel?
Voltaren and Flector Gel are topical anti-inflammatory gels which can provide relief from pain in joints and muscles. The active ingredient is diclofenac which is a non-steroidal anti-inflammatory.
Studies have shown that using Voltaren gel is better than using nothing for short episodes of pain, often from injuries like joint sprains or muscle strains (1). In fact the rubbing motion alone can reduce the sensation of pain.
Anti-inflammatory tablets (nurofen, advil, nagestic, herron blue) can also be taken by mouth and the amount absorbed into the blood is greater than from a topical cream, however, these tablets are associated with an increased risk of gastro-intestinal side effects like ulcers and bleeding, and are more likely to interact with other medications.
It’s been shown there is no difference between the effects of topical or oral anti-inflammatories when used for chronic conditions like osteoarthritis (2).
Ice Gel?
The main ingredient in Ice Gel is menthol. When applied, menthol creates a cooling sensation of the skin which can reduce the perception of pain for up to 30 minutes (3).
As Ice Gel reduces skin temperature, the amount of blood flow to the area decreases, therefore, Ice Gel can be effective if you are trying to reduce bleeding and swelling (4), like in the instance of a ‘corked’ thigh. However, reducing blood supply to an area can delay the body’s normal healing processes.
Tiger Balm?
Tiger Balm is designed to provide relief from muscle and joint pain. Ingredients include camphor, menthol, cajuput oil, mint oil and clove oil. These herbs help create a sensation of warmth and increase blood flow to help heal and repair tissue. There is no evidence supporting the use of Tiger Balm.
Arnica?
Arnica cream is derived from a plant, and has been used for the treatment of bruises, aches, sprains, insect bites, muscle pain and arthritis. The efficacy of arnica is hotly debated, and results from trials are mixed. Some studies state there is little difference between using arnica and topical anti-inflammatory gels like Voltaren Gel (5). While a different study reported that the use of arnica increased pain when compared with a placebo (6).
All topical gels should only be used externally on unbroken skin. Irritation of the skin may occur, including rash, itching or redness.
We would like to thank Catherine Burns (a fourth year Osteopathic student who capably runs our clinic on a Saturday) for her work putting this article together.
(1) Derry, S., Moore, R.A., Gaskell, H., McIntyre, M., & Wiffen, P.J. (2015). Topical NSAIDs for acute musculoskeletal pain in adults (review). The Cochrane Library, 6.
(2) Derry, S., Moor, R.A., & Rabbie, R. (2012). Topical NSAIDs for chronic musculoskeletal pain in adults. Cochrane Database Systemic Reviews, 12(9). doi:10.1002/14651858.CD007400.pub.2.
(3) Johar, P., Grover, V., Ropp, R., & Behm, D.G. (2012). A comparison of topical menthol to ice on pain, evoked tetanic and voluntary force during delayed onset muscle soreness. International Journal of Sports Physical Therapy, 7(3):314-322
(4) Topp, R., Ledford, E.R., & Jacks, D.E. (2013). Topical menthol, ice, peripheral blood flow, and perceived discomfort. Journal of Athletic Training, 48(2):220-225
(5) Melzer, J. (2007). Herbal arnica montana gel not inferior to ibuprofen gel in topical treatment of hand osteoarthritis. Focus on Alternative and Complementary Therapies 12(4):257-258
(6) Adkison, J.D., Bauer, D.W., & Chang, T. (2010). The effect of topical arnica on muscle pain. Annals of Pharmacotherapy, 44(10):1579-1584
The "cost" of bulk billing?

This might be controversial but I think it needs to be discussed. I have been prompted to write about the cost of health care services due to a recent increase in referrals from other health practitioners. This is great and we always welcome new referrals but it has presented a dilemma or two.
Many of the the new referrals come to us through the Chronic Disease Management Program (subsidised by Medicare) and the presenting patients are often surprised that we don't bulk bill our services. I think this is because most come from Bulk Billing GP practices and are used to not paying much (if anything) for medical services. Also, we have recently had a lot of people walk in off the street or ring on the phone to seek advice for their presenting complaint without actually making an appointment. As most will appreciate the latter is difficult to manage as we definitely do not like to consult on the phone or diagnose and treat in the waiting room.
There are many financial reasons we don't bulk bill but fundamentally we don't do it as it devalues the therapeutic relationship. Everyone should be entitled to health services and we offer concessions where possible but getting something for nothing seems to be an increasingly popular mentality when it comes to health.
There is a very big elephant in the room when it comes to bulk billing for service. A recent article in the Sydney Morning Herald noted the trend for poorer quality health care as the cost to the patient reduces. This is due to GP time management as it does not become cost effective to see patients for more time when they are being bulk billed. At Fairfield Osteopathic Clinic we will not sacrifice time with patients. Hence, we will not bulk bill.
There have been suggestions regarding modifying Medicare payment processes and this may have been what the failed Federal Coalition Government Medicare Co-payment plan tried to address. The bottom line is those practitioners that choose to provide longer consults and spend more time gathering history and performing examinations/treatment should not be penalised.
We will always try and keep the cost of our consultations competitive for the business we are in. This is always a delicate balancing act. Osteopathy Australia our national association continue to lobby for more provisions through Medicare for Osteopathic services so that we can provide that care to more patients patients from broader socio-economic backgrounds.
The Massage "Affect" on Anxiety and Depression

JUST GET A MASSAGE
I know many people feel that booking in for a massage is an indulgence. They wait for a gift voucher from a loved one, or save up once a year for their birthday.
Many benefits of massage are still disconcertingly uncertain but while everyone is discussing those, a somewhat proven benefit is its positive effects on mood (1).
Massage has been shown to:
1. reduce depression
2. reduce anxiety
ANXIETY AND PAIN
How often have you noticed your neck pain is at it's worst when you're under a lot of stress? It will build up and up until you finally lean over to pick up your toothbrush and 'bam' you can't move your neck.
Anxiety is a potent factor in all types of pain. And in the case of lower grade anxiety and depression, the kind we all seem to be living with every day, massage can make a valuable contribution to your well being.
MASSAGE TO INTERRUPT THE CYCLE OF PAIN AND IT'S EFFECT ON MOOD
Although the neurophysiological effects are complex, the simple negative cycle that emerges when people are depressed or anxious, is that it's hard for them to do anything when they feel miserable. As you continue to feel miserable, this leads to doing less, which in turn, leads to feeling worse.
There is a boatload of evidence to support enjoyable movement and exercise to improve mood but how about not getting to the point of feeling miserable or trying to find someone to help you crawl out of that hole?
Most massage therapists are pretty nurturing types of humans. They can provide a therapeutic support role through 'recovery' and encourage paced activity to incorporate self-management.
IS MORE MASSAGE BETTER?
A leading researcher in this field is Christopher Moyer PhD who is a behavioural scientist primarily interested in the role of massage therapy on anxiety and depression or the human affect.
I'll let him speak about the research he has accumulated on the subject about whether more massage is better:
"We made an interesting discovery concerning the effect of the treatment on the state of anxiety. When a series of massage therapy sessions was administered, the first session in the series provided significant reductions in anxiety, but the last session in the same series provided reductions that were almost twice as large. This pattern was consistent across every study we were able to examine, which strongly suggests that experience with massage therapy is an important predictor of its success, at least where anxiety is concerned. To put it another way, it is possible that the greatest benefits come about only when a person has learned how to receive massage therapy." (2)
SO STOP FEELING GUILTY
You can all stop feeling guilty. If you enjoy getting a massage then book one now and do something good for your mental health. Give yourself a pat on the back for being proactive about your wellbeing. Well done you!
(1) Christopher A. Moyer, PhD, Research Section Editor, IJTMB, Assistant Professor, Int Journal Therapeutic Massage and Bodywork. 2008; 1(2): 3–5. Published online 2008 Dec 15.
(2) Moyer CA, Rounds J, Hannum JW. A meta-analysis of massage therapy research. Psychol Bull. 2004;130(1):3–18.
Relief from Low Back Pain

The "astronaut position" can be really helpful to relieve nagging low back pain
A top recommendation I give to people for acute or persistent low back pain tends to be a slight variation on the traditional Alexander Technique ‘semi supine’ or ‘constructive rest’ position. I’ve heard it called many things through the years including ‘the astronauts’ position.
I heard about it twenty years ago when my mother started lying in this position at home for her niggling low back discomfort. My Dad thought it was another women’s lib type of thing to accompany her afro, it was the early 80s and she was on the verge of discovering psychoanalysis. All that aside, she found it very helpful and has continued the practice, as required, for over thirty years.
Unlike many people today, my mother was quite good at recognising she needed to take ten minutes out from her day. I wouldn’t consider her schedule hectic compared to the modern working mother but even tennis days, canteen, extensive household duties, and coffee catch ups can take their toll.
Exactly what to do
Traditionally, semi supine is taught with no support under the legs but I often regress the position as many people struggle to relax while holding their legs in place.

Constructive Rest position

Regressed Position
Put your phone, book, work, television, computer, partner and children aside.
Lie on your back on a carpeted floor, or similar, preferably with with your calves resting on the couch or a coffee table so your knees and hips are bent to approximately 90degrees.

Folded towel to support neck if required
Most people need support under their head - use a small firm pillow or a folded towel (traditionally Alexander Technique recommends a book or two so you can achieve the ‘perfect’ height for comfort - paperbacks can be surprisingly comfortable)

Hands loosely folded across abdomen
Allow your hands to rest easily on your belly, chest or hips.
Time to quieten your mind
Mindfulness has moved beyond New Age and into the literature. One way to achieve mindfulness is to connect and check in with parts of your body.
- Let your neck be free
- Let your head, face, jaw and mouth slacken and melt
- Let your shoulders widen to the sides
- Let your back lengthen and widen
- Let your knees go out and away
- Let your bottom, inner thighs and pelvic floor release and soften
For how long?
Ten minutes seems to be a magic number but anything beyond five should be beneficial.
How do I get up?
Please don’t rush to answer the phone from this position. Your body has relaxed, your blood pressure has dropped slightly and your breathing is calm. Don’t ruin that with an adrenalin spurt and a fainting episode.

Knees into chest
Gently bring your knees toward your chest

Roll to your side
Roll to the side (PAUSE PAUSE PAUSE)

Come to sitting
Then come to sitting
Then come to standing
It works because:
You stop doing anything and relax.
Our nervous system can get a bit anxious and fired up, especially when we’re carrying pain. After a bit of lying down with less or no pain, it has a chance to calm down a bit. *
This will make you feel better.
Not just for emergencies
Semi-supine can be helpful anytime. Taking a break from the desk, music practice or study allows you to return to an activity, mentally refreshed and emotionally calmed.
We often forget we need to intermingle rest with activity. Let yourself take that rest - to benefit your body and your mind.
* There is also most likely multiple and as yet unknown and seriously complex neuro/mechanical/physiological responses that happens when we stop weight bearing and lie down on the floor in a strange position with pressure on the skin of our back.
Plantar Fasciitis - "Oh my aching feet!"

Plantar Fasciitis Help Sheet
Plantar fasciitis is a common and persistent type of repetitive strain injury causing foot arch pain with or without heel pain. Below are some practical tips to help manage the pain of plantar fasciitis.
Rest
· It takes as long as it takes – you need to properly rest until the tissue repairs. For most moderate cases, this will mean 1-2 weeks avoiding being on your feet (as best you can). After that, you need to spend the next few months gradually easing back into standing for long periods, walking or golf
· Maintain fitness with swimming or bicycling without toe clips
Ice
· A cheap, easy and safe way to help control pain short term
· Use an ice cube directly against the skin, moving it in slow circles for a maximum of 2 minutes. Another nice way of doing this can be freezing a plastic water bottle (filled with water of course) and rolling the arch of your foot over it. Ice massage!
· Allow the tissue to warm up before you repeat again, as often as you like
Contrast Bathing
· Force your tissues to adapt to sudden changes in stimulation and generate metabolic activity in the foot and leg
· Dunk your feet and leg in a good sized bucket of warm water for a minute, then into a bucket of cold water for a minute. Repeat at least 3 times in a row, as often as you want
Stretching
· Calf: heels on the ground, with toes against the wall or a door frame, and lean into the stretch OR the ball of the foot on a step and drop your heel down
· You need to do this with both a straight knee, and then with a bent knee to target all the calf muscles
· Plantar fascia: while sitting, hook a towel around your toes and pull toward your body until you feel a stretch
Mobilization
· Draw circles in the air with each foot. 20 circles per side, 3 times per day
· Point and flex the foot in the air. 20 in each direction, 3 times per day
Massage
· This can either be from a professional massage therapist or an osteopath or try it on your own
· You can spend up to twenty minutes a day massaging your feet and legs by rubbing gently over any tender points, or try rolling the base of your foot over a small ball
Night Splints
· Night splints hold the plantar fascia and calves in a gentle stretch overnight
· Either a soft or hard night splint will do the job
Arch Support and Heel Pads
· Shoe inserts from the chemist can help to offload the plantar fascia
· Find a comfortable pair of shoes, and try to avoid high heels as much as possible
· Heel pads are cheap and may help to cushion the impact of the heel on the ground
Some tips to reduce morning pain
· Start activating your muscles before you get out of bed. Draw 20 circles in the air with each foot before touching the ground
· Avoids stepping onto the floor barefoot or with no support. Make sure you have a supportive shoe to take your first steps with to give the foot a chance to start adapting to stress
CAUTION: Anti-Inflammatory Medications and Gels
· Use with caution as they can stop soft-tissues like muscles and the plantar fascia from healing, and they can have nasty side-effects on the gut
This is a summary of the amazing Plantar Fascia tutorial put together from a review of the current evidence on the treatment of the condition by the amazing Paul Ingraham from painscience.com
Here is a handy link for further information:
Stress and Pain

By now most of you would have seen the little incident with Mick Fanning (pro surfer) and a sizeable shark. If you haven't here is a little refresher
Thankfully there was no harm done to human (or animal). But the reaction and emotion of Mick Fanning is clear to see. There was an immediate flight or fight response as his muscles tensed and he was able to move very quickly and even punch the shark out of pure instinct. Immediately afterwards he is ashen faced as all blood is rushed to vital organs while the brain processes what is happening. To the brain there may have been injury and its main concern at that moment is keeping the body alive. This happens automatically.
The key message here is that stress is important. Very important. It may even save your life. But it is only good in small doses.
We live very strange lives now. We are constantly under pressure, creating stressful situations for ourselves through our personal and professional lives. Remember the last time you had to slam on the brakes in the car and the feeling immediately after that your heart was going to pound out of your chest? A sudden rush of hormones through the body (which help heighten senses) like adrenaline and cortisol causes muscle contraction and the heart goes crazy. The effects of an acute stress response are obvious but they are not pleasant.
Likewise, chronic levels of stress have much longer lasting and negative effects on the body:
- Muscles contract and stay tense, like they are on guard
- Risks of cardiovascular disease increase as the heart and major blood vessels become overworked
- Stress hormones have a negative effects on the liver which affects blood sugar reabsorption in some people making them at higher risk of type 2 diabetes
- male and female reproductive function can be severely compromised (1)
Then there is PAIN. In acute stress situations the stress hormones have an affect of dulling any pain. Just like a fight or flight situation when it is not really important to feel pain, it's all about survival. But excess levels of cortisol and adrenaline in chronic stress situations end up turning the volume up on pain and this can be very bad for long term health.
How do you think you would feel swimming around in J-Bay South Africa right now? Imagine you had to do that every day for the next week, month, or year. The "shark" is chronic stress and it can hurt you in more ways than one.
1. http://www.apa.org/helpcenter/stress-body.aspx
Five tips for a better night's sleep.

Sleep is a tricky topic. How many hours should we get? Seven, eight or nine? What has been the impact of television/screens/ipads? Should we sleep more like our ancestors in two big chunks (Bi-modal sleep)?
The overwhelming response from most people would be that they'd really just like a bit more of it.
Here's my top five tips to get a better night's sleep:
1. Stop unhealthy habits before bed
Finish eating or drinking at least two hours before you try to lie down.
Get off that computer or off the couch at least one hour before bed - seriously.
Check any nighttime medications* don't have caffeine in them.
2. Clear your bedroom of unhelpful items (make a checklist)
Get a blackout curtain if a street light shines in (it's not just for toddlers).
Is your room too warm or too cold?
Get rid of your shining alarm clock. No one needs to see the time in neon.
Turn off your mobile phone. I mean it.
Children and pets are warm, nurturing creatures but they don't always need to share the bed with you. We often get shoved into a cold corner of the bed to accommodate them. Restore your boundaries.
Is your mattress more than 8-10 years old? It might be time for an upgrade.
Do you love your pillow? (see my post on pillows)
Covers too heavy or restrictive?
Spouse or partner that is restless, noisy, or generates too much heat - um, acceptance?
Some medical conditions❡ interfere with sleep.
3. Do you love a daytime nap?
Do not daytime nap for more than 45 minutes
No napping after 3 pm
4. Exercise
A few surprises. A 2010 (1) study found people with no previous sleep difficulties slept better the night following exercise. But for people who had been diagnosed with insomnia, a fairly comprehensive study from 2013 (2) found people had to exercise daily and consistently for up to four months before there was a measurable benefit.
Put simply:
Consistently do a bit more physical activity during the day.
Expose yourself to bright light on waking – tell your body it's daytime.
Expose yourself to bright light in the afternoon to keep your body awake longer.
5. Consistency of sleep habits
Wake up at the same time every day - almost the hardest one to implement for anyone, especially an insomniac.
Develop a flexible before bed routine. It might include a warm shower or bath, meditation or a calming book.
In-bed routines - breathing techniques, progressive muscle relaxations (that's a whole other BLOG)
Reduce fluid consumption in the evening to avoid the need to wee all night.
(1) Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. Sleep Med. Oct 2010; 11 (9): 934-940. Kathryn J. Reid, PhD, Kelly Glazer Baron, PhD, Brandon Lu, MD, Erik Naylor, PhD, Lisa Wolfe, MD, and Phyllis C. Zee, MD, PhD
(2) J Clin Sleep Med. 2013 Aug 15;9(8):819-24. Exercise to improve sleep in insomnia: exploration of the bidirectional effects. Baron KG1, Reid KJ, Zee PC.
* Some medications that can interfere with sleep:
- Antihistamines: Benadryl (daytime drowsiness)
- Sympathomimetic Amines: bronchodilators and decongestants
- Antihypertensives and Beta blockers: Clonidine, Aldomet, Reserpine (daytime drowsiness)
- Steroids: Prednisone, dexamethasone
- Thyroid medications:
- Anti-epileptics and antipsychotics (daytime drowsiness)
- Parkinson medications: (daytime drowsiness)
- Stimulants for ADHD
- Anticholinesterase drugs for Alzheimer's
- Antidepressants: Prozac, Fluoxetine
- Analgesics: opiates, Tramadol, Ultram
- Chemotherapeutics: (nausea and vomiting)
- Diuretics: (frequency at night)
❡ Some medical conditions that can interfere with sleep:
- Respiratory disorders
- Cardiovascular disorders
- Gastrointestinal disorders
- Musculoskeletal pain and dysfunction (Book Online)
- Diabetes
- Renal disorders
- Prostate problems and small bladder causing urinary frequency
- Cancer
- Dementia
- Dental disorders
- Restless leg syndrome or Periodic Limb Movement Disorder (PLMD)
- Fibromyalgia (alpha wave intrusion)
NOTE: People who do shift work have special challenges as they consistently interrupt their diurnal rhythms. It is outside the scope of this post.
Strategies for a Healthy Winter - Guest Blog by Vicki van der Meer from Harvest Health
Move your body
Although there is a natural inclination to hibernate during Winter, it is also important to get regular exercise. As well as helping to stop us becoming sluggish and put on weight, regular exercise is important for our immune system
Wash your hands!
This may sound a little odd, or obvious, but regular hand washing is an effective strategy against contracting infectious illness. Special anti-bacterial soap is not necessary - just plain soap and water, with a proper scrub of the hands is all that's needed.
Warming foods

Ok, so it's fairly obvious that at some point I was going to mention food! During the colder months it's important to eat warming foods - this includes soups, casseroles, roasts. The root vegetables come into their own during winter and can form the basis of a meal by just cutting up and roasting in a pan, with some olive or coconut oil and a sprinkling of herbs such as rosemary. Garlic is immune enhancing and can be added near to the end of cooking lots of soups and casseroles for maximum benefit.
Orange
It is no coincidence that many of the vegetables in season now are orange, such as sweet potato, pumpkin and carrots. Orange vegetables are high in Vitamin A which is strengthening to the mucous membranes of the respiratory system.
Raw and green are good too
As well as enjoying the delights of winter comfort food, include some greens on a daily basis. Winter provides an abundance of green veggies - silverbeet, spinach, parsley, broccoli and salad greens all grow well. Some raw greens will give your body beneficial enzymes and fibre.
Drink warm drinks
Remember Enid Blyton books always contained the characters having 'steaming mugs of hot chocolate'?? A warm drink is very comforting. Beyond the usual tea and coffee, there is a whole world of herbal teas to try. Some good ones to start with are Licorice, Ginger, Dandelion root and Y.E.P (yarrow, elder and peppermint). The occasional hot chocolate is a winter treat to be enjoyed, not to feel guilty about!
My favourite immune nutrients
Vitamin C
Vitamin C is effective in preventing and treating common respiratory infections such as the common cold and the flu. It is most effective when taken right at the start of the infection, when you first suspect you might be ill. It is possible to take quite high amounts by taking small doses regularly over the day. Vitamin C is absorbed in the bowel, and maximum absorption is attained when taken in divided doses rather than one large amount.
Zinc
Zinc is an essential trace element that is involved in many aspects of immune function. It is essential for the normal development and function of many immune cells. Zinc lozenges are very useful at the start of a cold, and can be taken in conjunction with Vitamin C. Just be careful when taking Zinc, not to take it on an empty stomach as it can make you feel nauseous.
My favourite immune herbs

If taken early and often enough, the immune enhancing herbs can stop a cold from developing. At the very least they can lessen the duration and severity of a cold. My favourite ones are Andrographis, Echinacea, Elder and Ginger. They can be taken in tablet form or as liquid extracts. In order to be effective though, they have to be quality herbs taken at the right dose.
A cold or two over the winter months is to be expected. However, by taking care of yourself and boosting your immune system, you can make sure they are mild and not debilitating. Embrace the goodness of winter while it's here.
To discuss your health and how you can feel better this winter, have a consult with Vicki in person.
Make a booking on line at https://fairfieldosteo.cliniko.com/bookings
or call Fairfield Osteo Clinic on 9489 0981
Why Should I Get A Massage?

Massage reduces your pain
Research into massage is difficult to do but the little bit of imperfect evidence that exists shows massage can improve low back pain (1). Unsurprisingly, the research also suggests massage doesn’t permanently fix every person from their back pain forever. REALLY?!? I’m not aware of many things that do.
Massage makes us feel good
Massage, like all manual therapy provided by skilled therapists, creates general well being effects (these are called non-specific effects in research). This doesn’t mean they’re simple, in fact it’s the opposite, but somehow they are always overlooked as important. Feeling good should be the primary objective.
It’s no small claim that the imperfect evidence in support of massage has also shown to reduce depression and anxiety (2). With the right therapist, in the right environment. Perhaps not the twenty minute brutal attack-type massage you get at your local shopping centre.
Another consideration is whether you like your massage therapist. I'm sure intuitively you know this is important but once again it's effect is often underestimated. A positive relationship creates a therapeutic alliance and it makes a big difference in how much better you will feel and for how long (3).
Can’t I just go to that drive-through massage place?
You can get a massage just about anywhere, anytime.
I’m sure you’ve seen the huge number of massage outlets popping up on High St in Northcote, Thornbury and Preston.
And what about the massages available at Northcote Plaza or Northland Shopping Centre? What will you get for your money? What are your therapists’ qualifications? Are they cheaper than the massage you’ll get with a two (or three) year qualified, private health rebatable, massage therapist at Fairfield Osteopathic Clinic?
As a society we want something and we want it now. That seems to be why there has been an explosion of massage therapy “shops” open in shopping centres throughout Melbourne. When you can have your aching back, neck or shoulder massaged RIGHT NOW we somehow stop caring about what qualifications the person touching our aching body has.
The more painful, the better?
The plethora of places to get a massage has led some legitimate, qualified practitioners to provide painful, heavy handed treatments so people walk away feeling like something serious and something medical has happened.
I’ve had a few patients lately who tell me about their experiences (not at our clinic) where they’ve cried during the treatment. I question the therapeutic value of this for anyone.
So get back into your body.
We live in a world filled with mental activity, computers, phones, social interaction, driving, working and we forget to exist in our bodies. We forget to move, to leap and run with joy. One hour of thoughtful, educated massage from a caring practitioner can bring people back into their bodies. Suddenly, they are back within themselves, in the room, in the present and they can get on with the job of feeling better.
Don’t leave your body with therapists who are semi-skilled. The massage therapists at Fairfield Osteopathic Clinic have all trained for over two years and will work with you to meet your goals, whether you need support for your marathon training, or massage to help reduce your stress and anxiety.
You can book online or call 9489 0981 to schedule an appointment........RIGHT NOW! ; )
1. Daniel C. Cherkin et al. A Comparison of the Effects of 2 Types of Massage and Usual Care on Chronic Low Back Pain: A Randomized, Controlled Trial. Ann Intern Med. 2011 Jul 5; 155(1): 1–9.
2. Moyer. Affective massage therapy. Int J Ther Massage Bodywork. 2008. PubMed #21589715.Massage researcher and psychologist Dr. Christopher explains that the only truly confirmed benefits of massage are its effects on mood (“affect”)
3. Ferreira PH, Ferreira ML, Maher CG, Refshauge KM, Latimer J, Adams RD.The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Phys Ther. 2013 Apr;93(4):470-8.
The worrying trend of spinal surgery

About a year ago an investigative journalist exposed the worrying trend of spinal surgery in the United States through CBS news. It got some attention.
It turned out that in the decade between 2001 and 2011 spinal fusion surgeries performed in the US sky rocketed by 70%. This may have been partially attributed to an increase in medical technology and an ageing population. Regardless, the increase was alarming and by the year 2014 the US was spending $12 billion and performing over 480,000 spinal surgeries annually. Yes, you read that correctly. That is over 1 300 spinal surgeries a day. A lot in anyone's book. (1)
So what are the statistics for Australia? A fairly robust study was published in 2009 in the Australian and New Zealand Journal of Surgery . The numbers follow the same trend as the US. In the period between 1996 and 2007 lumbar spinal surgery (mostly for lumbar spinal stenosis) increased 167%! "Woah" I hear you say. We beat the US at something! This is not something to be too proud of I'm afraid.
The take home message from this research was that there were disproportionate numbers of spinal surgeries being performed in the private sector, which they linked directly to private health insurance rebates. Why was this happening? You decide. (2)
Last week the Annals of Internal Medicine published a study showing that surgery for lumbar spinal stenosis was no more effective than manual therapy. There were some limitations to the study and it did acknowledge that some people do require surgery, which can be extremely effective for particular pathologies and neurological cases. Also, the study does not suggest that manual therapy is the answer to all pain associated with lumbar spinal stenosis but it is probably worth pursuing over costly surgery as the outcomes are often the same, if not better.(3)
There have been other randomised control trials (really high standard research) done comparing the effects of spinal surgery vs intensive rehabilitation for back pain, and spinal surgery vs cognitive behavioural therapy (a form of psychotherapy) for low back pain. Guess what? There was no difference in the outcomes for patients between the groups. (4) (5)
That leaves a bit of a confusing picture though. What do you do when presented with pain associated with lumbar spinal stenosis? In the first instance, short manual therapy treatment is by far the best course of action. Previous BLOG posts (see here) have looked at the importance of understanding your pain and being educated about the process of pain and recovery. Your Osteopath will always assess you appropriately and refer if there is anything that seems out of their scope of practice.
What is Osteopathy?

The word Osteopathy, along with the concept, was developed well over a hundred years ago. "Osteo" is clearly a derivation relating to "bone", but an Osteopath is much more than just treating bones. I'm pretty sure if it was developed now, a whole team of branding and marketing specialists might come up with a better name. It does have a fair bit to do with bones (as part of the overall musculo-skeletal system), but I don’t think there are many Osteopaths still out there who think we can use joint manipulation to cure serious disease. So whilst many theories have been culled from the original concept, the manual side of Osteopathy has evolved to help people with pain and provide professional advice in their recovery from injury or surgery.
A foundational principle, or perhaps the philosophy of Osteopathy, remains sound. Historically, Osteopaths were trained to treat the body, mind and spirit. In today’s speak, Osteopaths are trained to take a bio-psycho-social approach. Bio (body) pscyhological (mind) social (spirit) is at the very foundation of how Osteopaths think.
BIOLOGY (BODY)
We work with the body because we are manual therapists. This means we use our hands, our eyes and our brain to assess your body and use a broad range of hands-on techniques and movement therapies in order to modulate your pain and help you move better. Modulate in this context means to modify, hopefully in a positive direction, with the result being, you have less pain and movement is easier.
PSYCHOLOGICAL (MIND)
But where would we be without your brain, or ours for that matter. Our brain works with your brain. This doesn't mean we’re psychologists but it does mean we’re good listeners and we recognise the person standing in our room has a brain, a mind, a long history of lived experience; possibly trauma, happiness, an education. We work together with your brain, in countless ways, listening, discussing, educating and providing advice. We might challenge your default or resting postures, and significantly, we will educate you about pain and this might challenge the way you think about your pain.
SOCIAL (SPIRIT)
Osteopaths have historically also worked with your ‘spirit’. This is the part that can make people feel we’re a bit ‘out there’, a bit ‘crystal healing’, a bit ‘woo’. Once again, this aspect has an historical context. Osteopathy was developed when Science and Medicine didn't have answers for many horrible afflictions. Using leeches and ‘bleeding’ people was common practice.
Like medicine and the manual and physical therapy realm, Osteopathy has benefited from great leaps of understandings in Science over the last 100 years and especially research into neuroscience in the last 20 years.
Most people’s experience of pain improves when you are provided with nurturing environments, good education about pain and why it’s there, empowering explanations, and the knowledge of how to change their pain. This isn't pandering to the concept of a ‘spirit’ but it does recognise that people are complex creatures and appreciate being treated as humans.
TODAY
Many practitioners, whether medical or manual, still practice within a biomedical model in which they tend to treat just the anatomical aspects of a problem. “Here take some ibuprofen”, “You need to see me forever every four weeks to be truly healthy”, “Let’s strengthen your core to really solve the problem”, “Stand up straight”. They often ignore the other human aspects that might be contributing to the problem, including the most important part that runs every single aspect of our mind and body, our brain.
And we don’t forget the basics either. We are very qualified to rehabilitate post-surgical or post-injury movement dilemmas. That's our bread and butter.
At Fairfield Osteopathic Clinic, our Osteopaths meet with you for up to an hour the first time you come in, in order to grasp the whole picture.
Pillow, pillow on the bed, which is the best one for my head?

Which pillow shall be crowned in glory?
I am frequently asked about pillows. Most people who ask me ‘Should I get a new pillow?’ have arrived seeking treatment for a sore neck, insomnia or morning headaches. They don’t like their current pillow and have at some point flung it across the room in frustration. They may have paid a lot of money for one or many different kinds of pillows.
What is the perfect pillow?
I’m sorry, but I’m here to disappoint you, there is no perfect pillow. On a good day or given enough time, you can adapt to nearly anything. Over the last hundred years or so humans used rocks, horse hair and straw to help us sleep comfortably through the night. Before that we slept mostly on the ground, bereft of any pillow.
If we tried that now, out of the blue, then you’d be much like my twenty-four year old osteopathic colleague, Whitney, who recently went camping in Ballarat and slept on the cold hard ground, with only a thin, inadequate mat between her and the dirt. She was complaining this morning of sore shoulders, sore hips and an aching low back. Her whole body was yelling at her to march herself right back home to sleep on her $2000 mattress and contoured feather pillow. Unbelievably, she hadn’t spent any time at all progressively sleeping on less comfortable surfaces over the preceding weeks to get her body prepared for her camping experience. And really who would do that?
Our bodies and the bones, ligaments and muscles that make them up, respond to the activities that we ask of them. If we ask them to sleep on an extremely comfortable, forgiving surface every night then they’re just going to find it a bit of a struggle adjusting to a hard, cold, dirt floor. Your discomfort is not in your imagination.
So back to the person asking me about the perfect pillow. The one who has a sore, tight neck and shoulders and is struggling to adapt to anything. What do I tell them?
Your pillow is a support device.
Your pillow is there to provide support - it’s an orthotic for your head and neck.
A pillow that is unforgiving and asks you to adapt should be pushed to the side. It is meant to provide comfort and adapt to what you need, not the other way around.
This is not a sales pitch but we do sell a pillow at the clinic and it is the one I recommend to people if they’re genuinely in the market for a new pillow. It has a contoured cotton cover stuffed with polyester fill. The reason I like it is simple. It’s adaptable. It has a zip on one end that you can pull out stuffing or put more in as the polyester filling loses it’s ‘lift’. At night, you you can move the stuffing around if you punch it, or shove it into the headboard to make it higher when you roll from your back to your side. And in a couple of years when the filling bunches up and is full of saliva, dead skin and microscopic creatures, you can pull out the stuffing, wash the cover, stuff some new stuffing in and start again.
The Massage (Lacrosse) Ball - Best $8 You Ever Spent

I love these little balls. They’re cheap and they travel well. Recently, I had a client who took one on a bus tour to the Czech Republic. She took it to combat her mid back tightness and by the end of the trip all her travelling companions were impressed with it’s effectiveness.
Most people use it for ongoing tightness or a deep aching discomfort. They rarely like using it for acutely tender, sharp pain and I would not recommend using it for that kind of pain.
People often describe tightness building up over time, weeks or months that has rather suddenly turned into pain, like it has reached some kind of tipping point of tolerance and there is no turning back - not without a beach holiday, some meditation or some hands on therapy. Bring on the ball.
But how does it work? It has a local tissue effect due to the compress and decompress movement and also a nervous effect due to the DNIC approach that Todd Hargrove, a Feldenkrais practitioner from the US, writes about eloquently in this BLOG post from a couple of years ago. Using a massage ball is essentially the same approach:
http://www.bettermovement.org/2013/how-does-foam-rolling-work/
My disclaimers about it’s use are simple:
Use it for a maximum of 90 seconds in one location - nothing much changes after that and you’ll more likely cause injury.
Compress and decompress - that way you’re having a local tissue effect (squeezing and releasing the muscles) and you’re less likely to cause an injury.
Use it only every second day. That way you won’t build up a tolerance to the hard little sucker and start bruising yourself.
I recommend it for the big muscles down either side of the spine, the gluteal (buttock) region and the trapezius muscles.
Here is a little demonstration video we put together to help you get started.